Metabolic Health
Metabolic Syndrome in Functional Medicine
A Root-Cause Approach to Insulin Resistance, Inflammation, and Metabolic Dysfunction
Metabolic Syndrome in Functional Medicine
A Root-Cause Approach to Insulin Resistance, Inflammation, and Metabolic Dysfunction
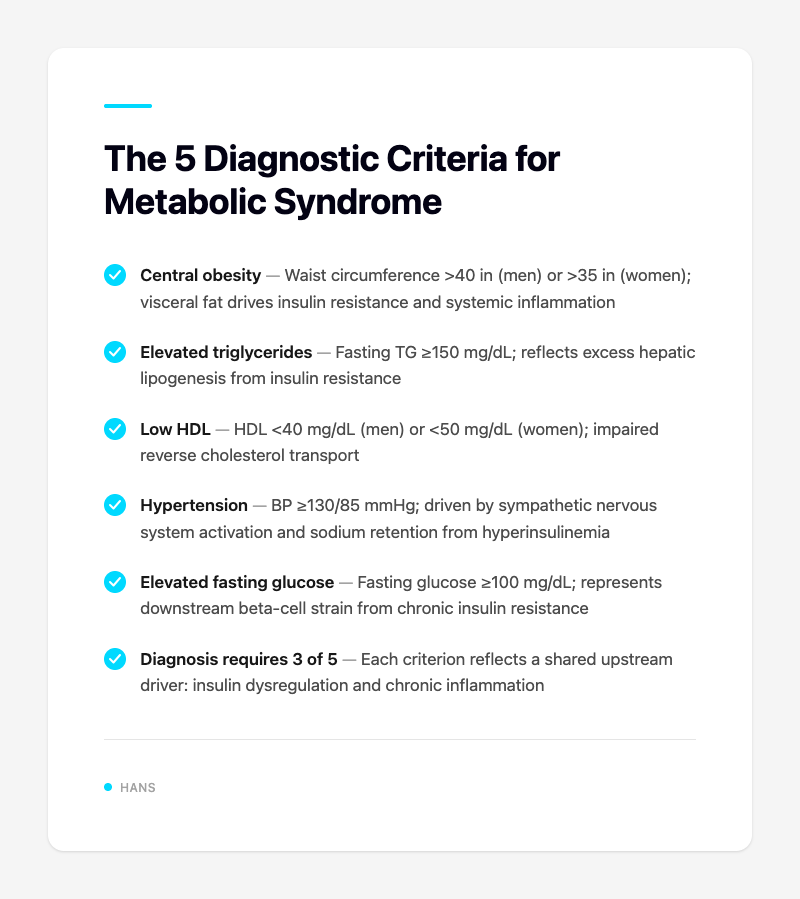
What is metabolic syndrome—and why does it matter in functional medicine?
Metabolic syndrome isn't a single diagnosis—it's a cluster of interconnected dysfunctions that significantly increase cardiovascular disease and type 2 diabetes risk. Conventionally, it's defined by the presence of three or more of: elevated triglycerides, low HDL, hypertension, fasting glucose elevation, and central obesity.
But functional medicine asks a different question: What's driving these abnormalities in the first place?
<<<<<<< HEAD
=======
65abf4f0 (vault backup: 2026-03-03 23:01:14)
The answer typically involves some combination of insulin dysregulation, chronic inflammation, gut dysfunction, adrenal fatigue, and environmental toxin exposure. Rather than managing individual biomarkers in isolation, FM practitioners look upstream—at the underlying patterns connecting them.
Which labs should I run to assess metabolic syndrome comprehensively?
Standard lipid panels and fasting glucose tell you part of the story. For a functional medicine workup, you'll want:
- Fasting insulin and HOMA-IR — often elevated long before fasting glucose or HbA1c rises
- HbA1c — gives you a 90-day glucose average
- Lipid panel with particle size — LDL particle number and pattern (Pattern B) matter more than total LDL
- High-sensitivity CRP (hs-CRP) — marker of systemic inflammation
- Uric acid — often elevated in insulin resistance
- GI-MAP or similar — to assess gut dysbiosis and intestinal permeability (zonulin, lipopolysaccharides)
Advanced practitioners may also consider: fasting adiponectin, leptin, oxidized LDL, and urinary organic acids for mitochondrial function assessment.
"Your patient with 'normal' cholesterol but fasting insulin of 22 μIU/mL has metabolic dysfunction—regardless of what their lipid panel shows."
How does the 5R Protocol apply to metabolic syndrome?
The 5R Protocol (Remove, Replace, Reinoculate, Repair, Rebalance) translates beautifully to metabolic patients:
- Remove — Inflammatory foods (gluten, dairy, processed sugars, seed oils), alcohol, and food sensitivities identified through testing or elimination
- Replace — Digestive enzymes if gut function is compromised; adequate fiber intake
- Reinoculate — Probiotics (species-specific: Lactobacillus reuteri, Bifidobacterium spp.) to support the gut-metabolism axis
- Repair — L-glutamine, zinc, quercetin, and butyrate to restore gut barrier integrity
- Rebalance — Sleep, stress management, targeted exercise
This approach addresses the gut-metabolism axis—where gut dysbiosis and elevated zonulin contribute directly to systemic inflammation and insulin resistance.
Which supplements have the strongest evidence for insulin sensitivity?
Here's what the literature supports:
| Supplement | Dose | Key Mechanism | Evidence |
|---|---|---|---|
| Berberine | 500mg BID | Activates AMPK, improves insulin sensitivity | PMID 31991469 (meta-analysis: HbA1c reduction comparable to metformin) |
| Myo-inositol | 2g BID | Insulin signaling, glucose transport | PMID 35189579 (systematic review—PCOS and metabolic markers) |
| Chromium | 200-400mcg daily | Enhances insulin receptor activity | Mixed evidence; may help in deficient states |
| Alpha-lipoic acid | 300-600mg daily | Antioxidant, improves insulin sensitivity | Supports peripheral glucose uptake |
| Omega-3s (EPA/DHA) | 2-3g combined | Anti-inflammatory, lowers triglycerides | PMID 30000812 (reduces triglycerides, improves HDL) |
| Vitamin D | As needed to reach 50-80 ng/mL | Modulates inflammation, insulin signaling | Deficiency common in metabolic syndrome |
| NAC | 600mg daily | Glutathione precursor, reduces oxidative stress | PMID 33126547 (improves fasting insulin and HOMA-IR) |
Clinical pearl: Berberine and myo-inositol work synergistically. Many practitioners combine them with alpha-lipoic acid for patients with significant insulin resistance.
What lifestyle interventions outperform medication alone?
This is where functional medicine shines. Evidence increasingly shows that lifestyle modification addresses the root causes more effectively than pharmacotherapy:
- Time-restricted eating (12:8 or 14:10 window) — improves insulin sensitivity, reduces fasting insulin, and supports circadian rhythm
- High-intensity interval training (HIIT) + resistance training — HIIT improves insulin sensitivity more efficiently than moderate cardio; resistance training preserves lean mass
- Sleep optimization — Sleep deprivation raises cortisol, increases hunger hormones (ghrelin), and worsens insulin resistance. Aim for 7-9 hours; address sleep architecture if needed
- Stress management — Chronic cortisol elevation drives visceral fat accumulation and gluconeogenesis. Adaptogens (ashwagandha, rhodiola) can support HPA axis regulation
"A patient who normalizes their sleep and implements HIIT three times weekly will often see better metabolic improvements than one relying on medication alone—without the side effects."
Case Example: 48-Year-Old Female with Pre-Diabetes and Weight Loss Resistance
Presentation:
- 48F, BMI 31
- HbA1c: 5.8%
- Fasting insulin: 18 μIU/mL (elevated)
- hs-CRP: 3.2 mg/L (moderately elevated)
- Chief complaint: "I can't lose weight no matter what I do"
Functional Medicine Approach:
- Removed inflammatory foods — gluten, dairy, processed sugar eliminated for 30 days
- Supplement protocol — Berberine 500mg BID + Myo-inositol 2g BID + NAC 600mg daily
- Time-restricted eating — 12:8 window (12pm–8pm)
- Gut restoration — GI-MAP revealed elevated zonulin and F. prausnitzii deficiency; targeted probiotic and butyrate support
- Lifestyle — Sleep optimization (targeting 7.5 hours), stress support with ashwagandha
Outcomes at 6 months:
- HbA1c: 5.4%
- Fasting insulin: 9 μIU/mL
- hs-CRP: 0.8 mg/L
- Weight: -14 lbs
This case illustrates how addressing multiple upstream drivers simultaneously—gut health, inflammation, insulin signaling, and lifestyle—produces results that isolated interventions rarely achieve.
Visual Resources
Diagram showing interconnected factors in metabolic syndrome: insulin resistance, inflammation, visceral fat, dyslipidemia, hypertension. Medical infographic style with connected nodes.
Horizontal bar chart comparing lab values before and after functional medicine intervention. Clean medical style, muted blue and green colors.
Visual layout of supplements for insulin resistance: berberine, myo-inositol, chromium, omega-3, alpha-lipoic acid. Organized on clean background with labels. Medical supplement guide style.
Quick Reference: Metabolic Syndrome Protocol Checklist
- Comprehensive labs (fasting insulin, HOMA-IR, HbA1c, lipid panel, hs-CRP, uric acid)
- Gut assessment (GI-MAP or similar)
- Remove inflammatory foods
- Core supplements: Berberine + Myo-inositol ± NAC
- Time-restricted eating protocol
- Exercise prescription (HIIT + resistance)
- Sleep optimization
- Stress management
Related Resources
→ Pillar: Metabolic Syndrome Functional Medicine Guide
→ Hub: Functional Medicine Protocols
Ready to stop re-documenting the same metabolic protocols from scratch?
HANS auto-generates condition-specific FM documentation—labs, supplement protocols, lifestyle plans, and patient handouts—so you can focus on clinical thinking, not paperwork.
References
Berberine for metabolic syndrome and type 2 diabetes: a meta-analysis. Front Pharmacol. 2020; PMID: 31991469.
Myo-inositol supplementation in metabolic disorders: systematic review. Nutrients. 2022; PMID: 35189579.
N-acetylcysteine improves insulin signaling and oxidative stress in metabolic syndrome. Endocr Metab Immune Disord Drug Targets. 2020; PMID: 33126547.
Omega-3 fatty acids and metabolic syndrome: effects on lipid profile and inflammation. Prostaglandins Leukot Essent Fatty Acids. 2018; PMID: 30000812.